
Malaria is a caused by transmission of a Plasmodium parasite, which are spread exclusively through Anopheles mosquitoes. There are four parasite species that differ in their lethality, so death rates are variable depending on parasite species and treatment availability. Even if an individual survives, malaria can lead to anemia, which is quite dangerous for pregnant women. Additionally, children who survive severe malaria can have mental disabilities.
 |
| Worldwide malaria transmission rates; from DPDx |
 |
| Current malaria risk in Kenya. from DataDredger. |
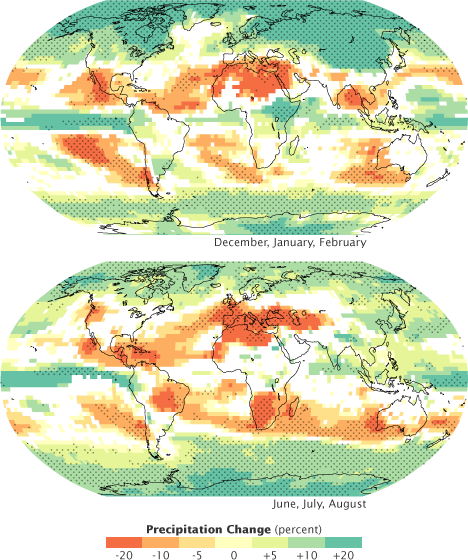
Less work focuses on the role of changes in precipitation in changing malaria incidence rates. Prior work shows that droughts tend to reduce incidence rates, and high rainfall increases Anopheles population sizes. However, uncertain predictions of changes in rainfall in Kenya make incorporating these predictions quite difficult. Most climate models predict a decrease in rainfall (see the first blog post), suggesting that rates of malaria will decrease, but it seems possible that increased variability in precipitation could change the seasonality of malaria infection.
Eradication of malaria is possible with aggressive prevention tactics. Up until the last century, malaria was common across the world, including Europe and North America, but was successfully eradicated, suggesting the same can be done in African countries such as Kenya. There have already been successes in parts of Africa, with frequency reduced by 50% in 1/3 of countries where malaria is endemic; this reduction is due in part to global health organizations such as the Global Malaria Action Plan, the Roll Back Malaria Partnership, and WHO.
Tactics to reduce incidence of malaria are fairly straightforward, and there is much room for improvement in Kenya. First, prompt diagnosis and treatment is critical; the most lethal strain of malaria is lethal within the first 24 hours. In the Lake Victoria area, 1/2 of parents do not seek treatment when their children under 5 years develop a fever, and only 1 out of 10 children is given a blood test for malaria. Two-thirds of medical facilities do not even have the capacity to diagnose malaria via a blood test. In terms of treating the disease, more than half the mothers in the coast area have not heard anything about the most common antimalarial medicine.
 |
| A woman and child underneath a mosquito net; from Healing Hearts. |
In addition to rapid diagnosis and treatment, use of insecticides and mosquito nets is critical to preventing malaria. Spraying residences with insecticides reduces the instance of malaria, but only 1 out of 10 children under 5 years sleeps in an insecticide-treated residence. The use of insecticide-treated bed nets to protect people from nighttime bites also drastically decreases incidence of malaria. However, the proportion of Kenyans owning insecticide-treated nets has stagnated since 2007, and in malaria-endemic areas, there is only 1 net for every 5 Kenyans (the nationally-recommended ratio is 1 to 2).
National efforts to prevent the spread of malaria with climate change have focused on improved prediction of outbreaks as a function of climate data, which is critical in an region of changing incidence rates. Improved prediction will allow healthcare providers to take preventative measures such as distributing nets or spraying for mosquitos, thus increasing the capacity for dealing with outbreaks in susceptible areas. For example, in the highland areas near the Mount Kenya region, where malaria has been rare historically, workers have focused on disseminating mosquito nets to people with little experience of the disease.
 |
| Administration of a malaria vaccine; from the Guardian Express. |
One of the most heartening advances in the fight against malaria in Kenya in particular and Africa in general is the recent development of a vaccine, which was tested in seven African countries, and may be ready for approval by WHO by 2015. This vaccine is effective against the most virulent Plasmodium parasite, but is not currently licensed for use as a malaria control tool.
Changes in precipitation and temperature with climate change will shift the distribution of malaria incidence in Kenya, with rates increasing the highland and decreasing in the lowlands. Given the relative unfamiliarity of highland Kenyans with this disease, as well as low rates of preventative measures, it is critical to develop effective preventative and mitigation strategies in these susceptible areas, both at the national and international level.














.jpg)

{kind=link}